Procedures
Cardiac Procedures
- Coronary Angioplasty
- Heart Bypass Surgery
- MICS CABG Surgery | Minimally Invasive Heart Bypass Grafting
- TAVI - Transcatheter Aortic Valve Implantation
- Aortic Valve Replacement Surgery
- Balloon Mitral Valvuloplasty (BMV Procedure)
- Device Closures - ASD/VSD/PDA
- Pacemaker Implantation
- CRT Implantation
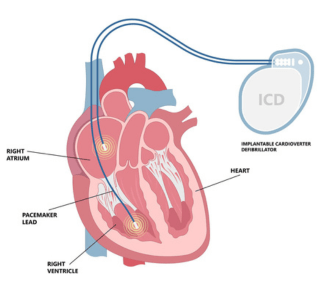
- ICD Implantation
- Hypertrophic Cardiomyopathy Ablation
- Thrombolysis