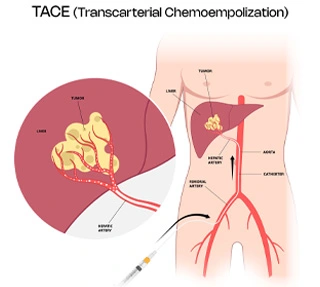
As the word suggests chemo embolization, which involves the placement of the chemotherapeutic drug inside the liver tumuor using the transarterial route (i.e through the femoral artery access in your groin). This is followed by embolization, which means blockage of the blood flow, so that the drug which has been placed remains inside and the blood flow to that tumour is also stopped to prevent tumour growth. The concept is that high dose of drug can be selectively placed inside the tumour for maximum effect and the blood flow to the tumour is also inhibited.
This procedure is recommended for tumours of the liver called hepatocellular carcinoma (HCC). It is now also approved for certain types of metastatic tumours and tumours of mixed-HCC etiology.
TACE is generally done for procedures wherein surgery is not feasible. Most procedures are done to keep the tumour under control and prevent tumour progression. They are predominantly done with an intent to increase patient life span and are not done with a curative intent. However, in certain specific conditions, TACE may also be done with a curative intent. These include: Focal tumours where in no other treatment is possible (patient not fit for resection or surgery). TACE can then be combined with other treatment modalities like tumour thermal ablation (either MWA or RFA). This is done for tumours between 3 and 5 cm in size. Here using both TACE and thermal ablation, curative intent can be achieved. TACE can also be done as a bridge to transplant. The final treatment for HCC is either resection or liver transplant. While the patient is awaiting transplant, TACE can be done to keep it under control. Here, it is used as bridge therapy.
With newer techniques and devices, it is possible to enter the smallest arteries of the tumours, thus depositing the drug only to the tumour and not affecting the liver. This is variable – depends on the operator and case to case.
Ideal treatment for liver tumour is either resection or transplant, because that is curative. Like said earlier, TACE is generally for preventing disease progression and improving life span. Rarely it is curative (as discussed above). When the option of surgery is out, TACE is your best bet. For extremely progressed tumours involving both the liver lobes and/or portal vein, even TACE may not be possible. In those circumstances only systemic palliative chemotherapy may be an option then. You need to be assessed by your doctor to see whether you are the candidate for TACE. This involves
Based on these parameters specially to see the liver status an make sure that the liver is functioning fine, you may be advised for or against TACE. A special doctor called an interventional radiologist (IR) performs TACE.
Contraindications for TACE Procedure
Patients in which the liver functions are grossly deranged, in cases with portal vein thrombosis and with poor liver profile (subjectively measured with the MELD, Child Pugh score) are not good candidates for TACE.
What is the chemoembolization drug and agent given?
Generally doxorubicin is given mixed with a special agent called lipiodol to deliver the drug. This is inserted through a special tube called a microcatheter inside the small arteries of the liver. Following this, the artery is blocked with small beads called polyvinyl alcohol (PVA) particels or gelfoam slurry.

Structural & Interventional Cardiologist
MD, DM, DNB (Cardiology)
Location - Ghatkopar
View profile
Vascular & Interventional Radiologist
MBBS, DMRD, DNB (Radiodiagnosis), FRCR, EDiR, EBIR
Location - Ghatkopar
View profile
Structural & Interventional Cardiologist
MD, DM (Cardiology), FSCAI
Location - Dadar
View profile