The thyroid gland is an endocrine gland located in your neck. The word endocrine means it controls the hormones of your body. This vital gland; through hormonal control, indirectly controls all the organs of your body. It plays a pivotal status in controlling your basal metabolism, sleep, heart rate, growth, bodily functions and overall development. Any lump or lesion developing within the thyroid gland is called a thyroid nodule. Thyroid nodules may be solid or fluid-filled i.e cystic. These nodules are very common in the general population and as per data can be present in roughly 1 of 3 individuals.
As stated above, thyroid nodules are very common and most are asymptomatic. However, every nodule needs to be evaluated. Your doctor would first examine you and ask for investigations. Most importantly, it is important to know whether the nodule is arising from thyroid or from a surrounding structure (i.e. extra-thyroid). An ultrasound (USG) is the best investigation to evaluate the thyroid nodule. This is required to know the size, location and nature of the lump or mass/nodule. Most thyroid nodules are benign i.e non-cancerous. You need not worry. Almost 95% are benign. Only a small percentage (around 5%) of thyroid nodules may be worrisome i.e are cancerous.
Most often, you won't even know you have a thyroid nodule as they have no symptoms. These are most likely incidentally detected or discovered during a heath check up. Rarely, your doctor may find it during a neck examination. In other cases, it may be picked up on a CT scan or ultrasound done for other reasons.
However, that said, large thyroid nodules may have symptoms. These symptoms include:
Diagnosis of Thyroid Nodule
If the nodule turns out to be cancerous or malignant
In this case, the most likely option is surgery or chemotherapy. This may be combined with radioactive Iodine therapy. You would require a mullti-disciplinary team of doctors for taking the right decision for you, this would include a medical oncologist, a surgical oncologist, an endocrinologist, an interventional radiologist and a pathologist. They would advise the next steps of investigations and treatment plan.
If the nodule turns out to be benign
It is a positive news if the nodule turns out be benign. If the nodule is small (<2 cm), nothing needs to be done. Only follow-up is required. A wait and watch policy may be offered. Every 6 months or yearly, an ultrasound may be suggested to make sure that the nodule is not increasing in size.
Some thyroid nodules are however pretty big and may cause symptoms. Even though the nodule is benign, since it is symptomatic, treatment may be required. This varies from case to case. Symptoms include:
1. The nodules may be felt – hard or painful
2. May be seen, often as a swelling at the base of your neck; causing cosmetic disfigurement.
3. They may press on your windpipe or esophagus, causing shortness of breath or difficulty during swallowing (i.e dysphagia or dyspnea)
4. In some cases, these thyroid nodules shall produce additional thyroxine, a hormone secreted by your thyroid gland. These are called autonomous or functioning nodules. The hormone produced by the nodule can cause something called as hyperthyroidism. Symptoms of hyperthyroidism include:
Unexplained weight loss
Increased sweating
Tremors
Nervousness
Rapid or irregular heartbeat
Overall, such symptomatic benign thyroid nodules require treatment.
Treatment options for a benign symptomatic thyroid nodule
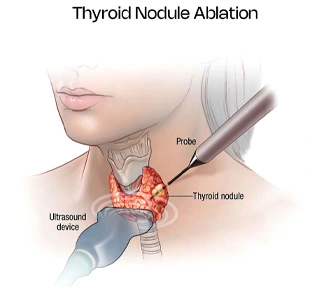
Conventionally, open surgery has been offered for benign thyroid nodules. This would involve removing the nodule and a part of the thyroid gland (a procedure called hemithyroidectomy) or the entire gland (total thyroidectomy). Surgery has its own issues: long term hormone supplementation and surgical complications. Hence, for such symptomatic benign thyroid nodules a treatment now offered is: percutaneous thermal ablation of the nodule.
“Percutaneous” means through the skin. The word ablation means destruction of tissue. “Thermal” means heat.
Therefore this procedure involved destroying the nodule using a special device through your skin with the help of heat.
Heat is given either in the form of radiofrequency energy (RFA) or microwaves (MWA). We have used RFA and MWA safely in other organs like the liver and lung for almost 20 years for destroying liver and lung tumours.
Thyroid RFA has been performed at specialist centres abroad for many years and more recently has gained popularity in India.
Benefits of percutaneous radiofrequency ablation compared to open surgery
As compared to open surgery, there are various advantages of thermal ablation of nodules:
Which doctor will be performing percutaneous thermal tumour ablation?
Image guided procedures require specialists doctors called Interventional radiologists (IR). These are specially trained medical professionals who performs image guided procedures. Every thyroid nodule work up eventually requires an multi-team approach: involving the interventional radiologist, endocrinologist and an oncologist/surgeon.
No procedure can be risk free. But since thermal ablation is a minimally invasive treatment option (MIT), risks are much lesser than open surgery. Serious complications are extremely rare. The main risk is hoarseness of voice on the post procedure follow up. This happens due to nerve injury. Even if this ensues, it is self limiting and generally recovers on its own over 1-3 months.

Structural & Interventional Cardiologist
MD, DM, DNB (Cardiology)
Location - Ghatkopar
View profile
Vascular & Interventional Radiologist
MBBS, DMRD, DNB (Radiodiagnosis), FRCR, EDiR, EBIR
Location - Ghatkopar
View profile
Structural & Interventional Cardiologist
MD, DM (Cardiology), FSCAI
Location - Dadar
View profile