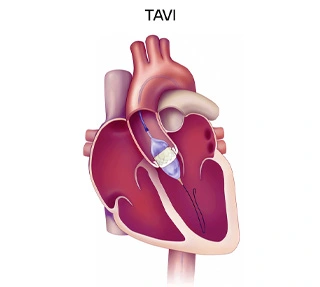
TAVI or transcatheter aortic valve implantation is a minimally invasive percutaneous procedure done to treat a narrowed aortic valve of the heart. Aortic valve is one of the four valves of the heart which enables the flow of blood from the heart into the aorta (main vessel of the body) and through it to the entire body. Most common reason for the narrowing of the valve is ageing.
TAVI was first done by Dr. Alan Cribier in April 2002 in France. Thus the journey has evolved over 2 decades now.
Initially under general anaesthesia by surgeons, now it is regularly done by Cardiologists in Cath lab under mild sedation or even local anaesthesia.
The valve and its accessories have also evolved with time, and have gotten smaller in size which enables it to do get the procedure done through smaller sheaths in the groin arteries.
TAVI is an attractive alternative for elderly patients as:
SAVR is mainly done in patients who are young, i.e., younger than 65 years of age with no other major comorbidities.
Who is a Good Candidate for TAVI Procedure?
Any candidate who has been diagnosed with severe aortic stenosis (i.e., aortic valve narrowing) and is more than 65 years of age is a candidate for TAVI procedure. Occasionally, if a younger patient has many comorbidities and may have a high risk for open heart surgery, then they may also be a candidate for TAVI procedure.
Pre-Procedural Preparation for TAVI
Prior to TAVI, routine blood tests are done. ECG, echocardiogram, and usually a coronary angiogram are performed prior to the procedure.
Multidisciplinary Team Approach in Patient Evaluation
Once severe aortic valve narrowing is diagnosed, a heart team discussion is done which involves the cardiologist, a cardiac surgeon, and the patient and their relatives. Both the pros and cons of the TAVI and surgical AVR are discussed and put forth for the patient to choose which procedure they would like to proceed with.
Types of TAVI Valves, Selection Criteria & Their Durability
There are mainly two types of TAVI valves: Balloon-expanding and self-expanding ones. Balloon-expanding valves are mounted on the balloon itself and opened at the valve level, whereas the self-expanding valves are expanded at the valve level by self-opening with an inherent valve opening mechanism. Various valve companies have their valves available in India. Based on the patient characteristics and the CT scan measurements, the best valve suitable for the patient will be discussed by the cardiologists. Usually, the valves last for around 10-15 years, but it depends on the patient and inherent valve characteristics.
Step-by-Step Description of the TAVI Procedure
Usually, the TAVI procedure is done through the transfemoral access, but in some cases where this access is not feasible, alternative arteries like subclavian (arms), carotid, or aortic (neck) arteries may be used. In very occasional cases, transapical i.e., direct insertion through the heart may be performed.
Post procedure, the patient is shifted to the ICU for overnight monitoring of the heart rate as the procedure is bound to cause heart blocks.
There is very little recovery time needed post an uncomplicated procedure. Patients can walk the same day and can be discharged home the next day.
How long will it take to recover fully?
Usually some rest is advised at home for a few days post procedure, but after a couple of weeks, patients can resume their daily activities.
Are there any restrictions or activities I should avoid during recovery?
Post the procedure you should not drive a car for a few weeks as per your country's regulations. Groin care is needed for a few days post procedure, so you should avoid squatting down for a few days post procedure.
Short-term and long-term follow-up protocols.
Blood thinners are to be continued post procedure. Else no other specific treatment is needed post procedure. Regular echocardiogram screens are done for these patients. Firstly a pre discharge echo is done to see the valve parameters and then usually they are done yearly or earlier if there are any new symptoms.
Following main complications can occur during or post the procedure:
There are promising outcomes for the short and medium term post TAVI procedure. With rates better than surgical AVR. The success rates are getting better due to better valves and also the gaining expertise of the cardiologists.
Long term success rate of TAVI
Long term success of TAVI procedure is also good, though it may be slightly difficult to analyse as patients are usually elderly and may have many other comorbidities to make things difficult to evaluate. To put it in simple words, TAVI patients as they are old with many other diseases, may die from other causes as well.
Comparison of outcomes between TAVI and SAVR
In the short term, definitely the TAVI valves do better over the surgical AVR as it is less invasive and a procedure with fewer complications. Recent long term data for longevity of the procedure show similar rates of valve degeneration for both TAVI valves and bioprosthetic surgical valves.
Sometimes the CT characteristics or the patient per se may not be suitable for the TAVI procedure. For eg. the access may be an issue or occasionally the annulus may be such that it may be a very high risk for a TAVI procedure. Though these characteristics which may preclude the TAVI procedure are few.
Cost-effectiveness and Accessibility Issues
This is the main limitation in countries like India where the procedure expense is done by the patients themselves and is not presently state funded in most states. As a surgical AVR is usually a cheaper procedure presently, many patients may opt for the same even if they are better candidates for TAVI.

Structural & Interventional Cardiologist
MD, DM, DNB (Cardiology)
Location - Ghatkopar
View profile
Vascular & Interventional Radiologist
MBBS, DMRD, DNB (Radiodiagnosis), FRCR, EDiR, EBIR
Location - Ghatkopar
View profile
Structural & Interventional Cardiologist
MD, DM (Cardiology), FSCAI
Location - Dadar
View profile