Lower urinary tract symptoms or LUTS associated with benign prostatic hyperplasia include:
- Increased urinary frequency
- Recurrent urinary tract infections due to urine stagnation
- Recurrent fevers
- Nocturia or increased frequency of urination at night
- Poor stream or force of urine
- Feeling of incomplete voiding or incomplete emptying of the bladder
- Rarely due to backpressure changes, there may be obstruction of urine in the kidneys called hydronephrosis
- Dribbling of urine
- Blood in urine called hematuria (rare)
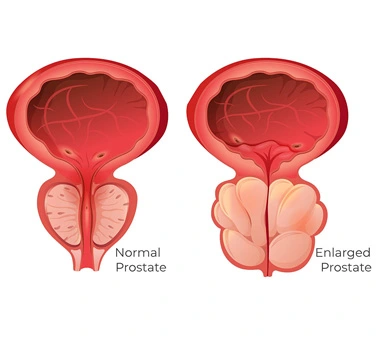
Why does the prostate enlarge in size?
As age advances, the prostate increases in size in most males, (especially those above 60) due to hormonal changes. Testosterone secreted from the testes is the main factor, which increases as age advances and causes gland enlargement.
What is the normal size of the gland?
Normally the prostate weighs 25 – 30 gm. An increase in size above that is taken as an enlarged gland. However, the size does not determine symptoms. Even a mildly increased gland may cause severe symptoms, while an extremely large gland may have no symptoms.
Is BPH a common problem?
BPH is very common in the adult male population above the age of 60. It is said that by age 90, 90% of people will have BPH.
Is BPH and prostatic carcinoma different?
BPH and prostatic carcinoma are two different conditions. BPH does not increase the risk of prostatic carcinoma. BPH affects the central gland, while prostatic carcinoma affects the outer peripheral gland. Symptoms may be similar, therefore malignancy with screening blood tests (PSA levels) should be done to rule out malignancy.