EVLT Procedure
Endovenous means from inside the veins. Therefore EVLT means ablating or burning the veins from inside using Laser.





Where Experience Meets Excellence in Vascular Care

Vascular Services at HVS Hospitals in mumbai are specialised services which are generally offered via small clinics across the country. Our Vascular department is an attempt to elevate the services with provision for best infrastructure including fully equipped ICU and dedicated specialists. We take pride in ourselves of having a team of experienced Vascular & Interventional Radiologists in Mumbai.
Vascular techniques in modern medicine are gaining recognition for being effective and less risky. At HVS hospitals, we are introducing the gold standards treatment in fully equipped hospital facility to ensure best results for patients.
Our dedicated team of vascular specialists are here to provide you with world-class care. With extensive experience and specialized expertise, our consultants are committed to delivering personalized and comprehensive treatment plans.


Vascular & Interventional Radiologist
MBBS, DMRD, DNB (Radiodiagnosis), FRCR, EDiR, EBIR
Location - Ghatkopar
View profile
Vascular & Interventional Radiologist
MBBS, MD, FVIR
Location - Borivali
View profile
Vascular and Interventional Radiologist
MD Radiodiagnosis, FVIR
Location - Thane
View profile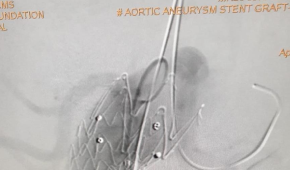
A 55 years male patient with history of sudden abdominal pain followed by syncope was rushed to the hospital. CT abdomen + angiogram s/o fusiform dilatation of the abdominal aorta. Eccentric thrombus along the left lateral wall, showing further extension along the aortic bifurcation to involve bilateral common iliac arteries may represent thrombosed aneurysm/ intramural hematoma.
The findings most likely represent a ruptured & thrombosed fusiform aortic aneurysm. On receiving patient in ICU he was in hypovolemic shock with poor general condition. Blood pressure on admission was 80/40 mmHg, with a heart rate of 120/min. Physical examination of the abdomen was soft with tenderness in the left lower quadrant. No pulsatile mass was present. Femoral pulses were palpable symmetrically. Nor Adrenaline infusion started. Routine investigations sent and volume resuscitation was done with Blood transfusion followed by Fresh Frozen Plasma. Hb was 6.5 with an INR of 1.2. Rest routine reports were within acceptable range.
Patient was stabilized and shifted to Cath Lab for Abdominal Aortic Stenting.
She underwent Abdominal Stenting with Graft by a team of Interventional Radiologists & Cardiologists. Post procedure PCV transfused with Hb of 8.0. There was no further drop in Hb and rest of hospital stay was uneventful and patient discharged on POD 5.

A 70 years male was admitted and diagnosed with abdominal aorta aneurysm for planned abdominal aortic aneurysm stenting. He had history of low back pain for 2 years. His Follow up scan showed increase in size of Aortic Aneurysm with rapid progression of disease in Right Iliac artery. Considering his advanced age and co morbidities, patient was not willing for surgery and opted for minimal intervention.
After detailed evaluation patient underwent Abdominal Aortic stent grafting under general anaesthesia. Patient tolerated the procedure well and shifted to the ICU. All invasive lines removed gradually. He was treated with IV Antibiotics, LMWH, DAPT, Statin, Beta blocker and other supportive measures. The patient's postoperative course was uneventful and he was discharged on postoperative Day 4 with no renal impairment.
Procedure/Surgery Name: Geniculate Artery embolization for Recurrent Hemarthrosis
Doctors: Dr Bhavesh Arun Popat, Dr Karan M Anandpara
A 72 years old male
Comorbidities: Morbidly obese, poorly controlled diabetes, hypertensive, previous H/O CABG.
Complaints: Bilateral knee pain, joint aches and soreness (left>right knee).
Pain after joint overuse.
Reduced physical activity and quality of life.
Local knee tenderness +.
X ray bilateral knee s/o bilateral osteoarthritic changes (left more than right).
H/O left sided recurrent hemarthrosis for which percutaneous USG guided aspiration of fluid done outside.
USG local part suggestive of left sided hemarthrosis – hyperechoeic fluid with septations in the left knee joint cavity.
MRI done s/o changes of severe osteoarthritis with left sided hemarthrosis
Pain not relieved by conservative medical management i.e. by anti-inflammatory drugs or corticosteroids.
Not relieved by intra-articular steroid injection.
Not a candidate for joint replacement/arthroplasty in view of significant medical comorbidities, contraindications for general anaesthesia and patient’s refusal for knee arthroplasty.
Planned for Left sided Geniculate Artery Embolization in view of recurrent hemarthrosis and left joint pain.
Procedure under local anesthesia. Groin prepared.
Left Common Femoral Artery antegrade access.
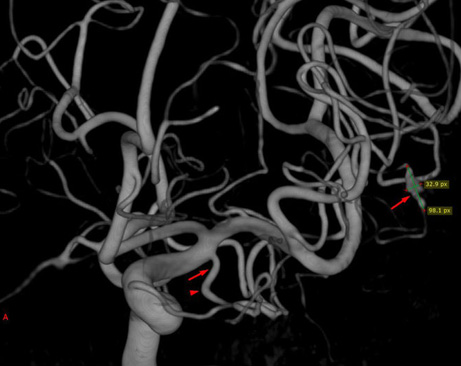
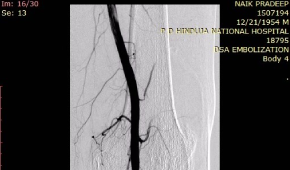
DSA Angiogram done which showed hypertrophied superior and inferior medial geniculate arteries.
Synovial vascular blush noted.
Super selective cannulation of the superior and inferior geniculate arteries done using Progreat microcatheter.
Embolization done with PVA particles.
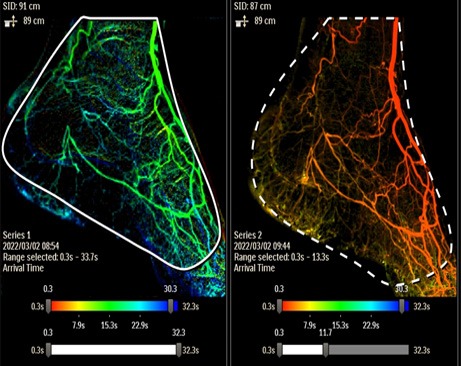
Post procedure DSA showed reduction in the synovial vascularity. Reduced arterial blush noted.
Sheath removed by manual compression.
Patient discharged on same day.
Significant reduction of pain on 1 and 3 month follow up.
Geniculate artery embolization (GAE) reduces pain of osteoarthritis by decreasing the vascular supply to the hypertrophied and inflamed synovium and has a role in cases of recurrent hemarthrosis.
It is safe, effective and minimally invasive.
No cuts, no stitches are required.
It can be Performed under local anesthesia.
No general anaesthesia needed.
It is a day care procedure with a same day discharge.